

WHAT IS CARPAL TUNNEL SYNDROME (C.T.S.)?
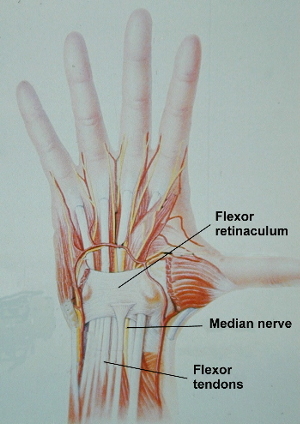
It is a painful disorder of the hand caused by excess pressure on the Median nerve as it passes through a tunnel at the wrist. The tunnel is formed by a tough membrane (Flexor Retinaculum) that makes a "roof' to a natural arch produced by the carpal (wrist) bones. The Flexor retinaculum keeps the tendons and nerves that pass under it in place & provides protection for the nerve. If structures in or around the tunnel swell then excess pressure on the nerve may cause nerve dysfunction.

Cross Section of the Wrist

WHAT CAUSES C.T.S.?
Often many factors play a role. One may have many factors but no symptoms of the condition and then one day develop the symptoms. The activity or factor which precipitated the symptoms may therefore act as “the last straw”. In many cases no obvious precipitant is identified and the condition arose because one got a little older.
- Obesity: - Best predictor of developing CTS
- Age: - (30-60) - In men the incidence increases with age. In women the peak age is between 30 & 60 years.
- Gender: - Female > male (3:1)
- Genetic: - often runs in families (small tunnel)
- Diabetes
- Family history of Diabetes (1/4)
- Pregnancy
- Post menopausal (Hormonal)
- Fluid retention
- Smoking (reduces blood flow to nerve)
- Alcohol: - lifetime intake is more important than what one is drinking at the particular time that the symptoms arose.
- Hormones: - e.g. under-active Thyroid
- Arthritis - e.g. Base of thumb or Scapho-trapezial
- inflammatory e.g. Rheumatoid
- Wrist fractures (Recent or Old)
- Neck Problems (Double crush)
- Kidney disease
- Activities: - Prolonged posture
- Renovating, Pruning garden, Sport
- Work:
- Highly repetitive + Highly forceful +either:
- Cold environment e.g. Butchers
- Excessive vibration stress e.g. Timber cutters
- Typing (NOT Associated with increased incidence of condition)
In a Scandinavian study of over 2500 patients the prevalence of CTS decreased with increased hours spent on the computer each day.
No Keyboard use 5.2%
Low ( <1hr / d) 4.9%
Moderate ( 1 – 4hr / d) 2.9%
Highest ( > 4hrs / d) 2.6% It seams that Intensive keyboard use lowers the risk of CTS
I. Atroshi et al Journal Arthritis and Rheumatism’Nov 2007
See also article on this condition by Sonja Falkiner & Dr Stuart Myers on this subject. Aust & NZ Journal of Surg. 72 (3). March 2002. 204 - 209
WHAT ARE THE SYMPTOMS?

The symptoms are very variable but usually include tingling and numbness in the hand. The little finger may be normal.
Pain may shoot up the arm from the wrist. The fingers may feel swollen. The pain and tingling are usually worse at night and may cause you to wake from sleep. It may result in weakness, clumsiness or loss of dexterity in the hand. It may be difficult to pick up small objects.
It may be relieved by shaking the hands or hanging them over the side of the bed.
DIAGNOSIS:
The diagnosis is usually straight forward and is made after eliciting a typical history (as above) and an examination.
Sometimes nerve conduction tests are performed if the diagnosis is unclear.
At times it may be difficult to determine if the nerve crush is occurring at the wrist or in the neck. An injection of Cortisone into the tunnel may help differentiate between these 2 causes of nerve compression.
In Diabetes and some similar conditions it is sometimes unclear whether the nerve dysfunction is due to pressure on the nerve, chemical damage to the nerve or lack of blood flow to the nerve. Again a Cortisone injection may be of assistance. A positive response to other treatment modalities (e.g. a wrist brace) may help confirm the diagnosis.
WHAT ARE THE RISKS?
It is usually not a serious problem. If the symptoms are present for a long time or the numbness becomes constant (i.e. present night & day) then it may cause permanent nerve damage. This may cause permanent weakness and numbness in the hand.
WHAT IS THE TREATMENT?
- Identify treatable causes for the condition
- Activity Modification
- Night Splints: - OAPL wrist brace holds wrist straight & opens up the tunnel
- Can be obtained from the physiotherapist or from a chemist
- Weight loss & Fitness training
- Stop smoking
- Cortisone injections
- Fluid tablets (occasional)
- Operation: - Involves cutting the membrane (Flexor retinaculum) to create more space in the tunnel for the nerve
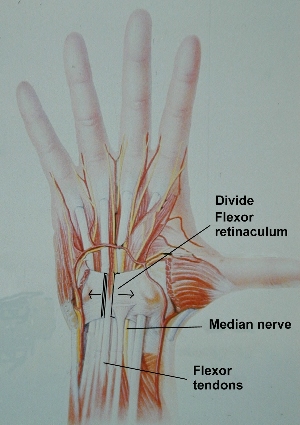

Surgery:
It is indicated in those patients in whom non-operative treatment has failed to eliminate their symptoms & when the symptoms are severe or if there is permanent numbness or muscle wasting in the hand.
1. Open
2. Endoscopic More information
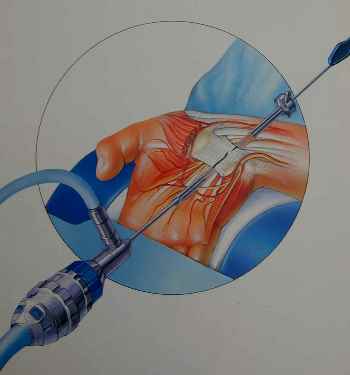
Results are the same for open or endoscopic release after 6 months but patients recover on average 3 - 5 weeks faster using the endoscopic technique (see separate section on Endoscopic Carpal Tunnel release).
The operation can be performed under local or general anaesthetic & requires admission to hospital for 1/2 day.
PROS & CONS OF SURGERY
Carpal tunnel release is usually very effective in relieving the symptoms of carpal tunnel syndrome in 95% of cases.
Recovery periods are extremely variable.
- If the symptoms are only present at night then many people notice resolution of their symptoms immediately after the operation.
- If the numbness is constant then the sensation may never fully recover or may recover over a period of 9 - 12 months.
Wasting of the muscles at the base of the thumb may never fully recover.
The major problem with the surgery is persistent weakness or aching pain in the base of the hand that may take about 3 months to settle down (Pillar pain). About 10% of people notice some permanent weakness or pain in the hand following the operation. While this is not a major issue for the majority of people if you were a heavy manual worker this could potentially be career ending.
Complications (rare):
- bleeding
- infection
- nerve, tendon or artery damage
- stiffness
- regional pain syndrome (0.5 - 1.0%)
- pain
- swelling
- stiffness
- colour change , sweating
- Recurrent Carpal Tunnel syndrome is possible but very uncommon.
If you are at all concerned or have any questions feel free to discuss them with me prior to the surgery.
LAST UPDATED ON SUNDAY, 27 FEBRUARY 2015