WHAT IS Cubital Tunnel Syndrome?
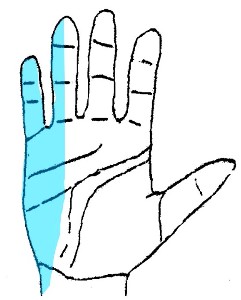
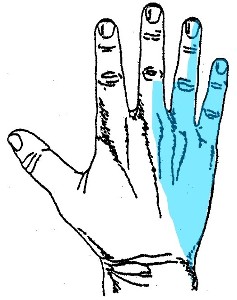
- “Cubital tunnel Syndrome” is where there is compression of the Ulnar nerve at the elbow causing numbness & tingling extending into the ring and little fingers, forearm pain and later weakness.

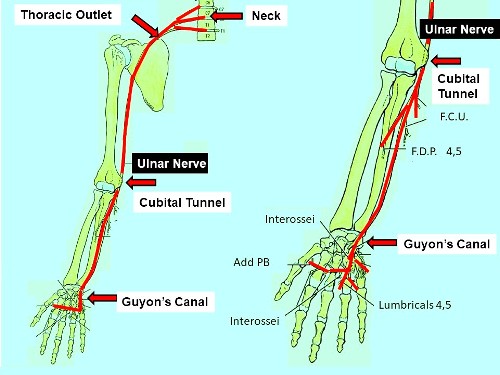
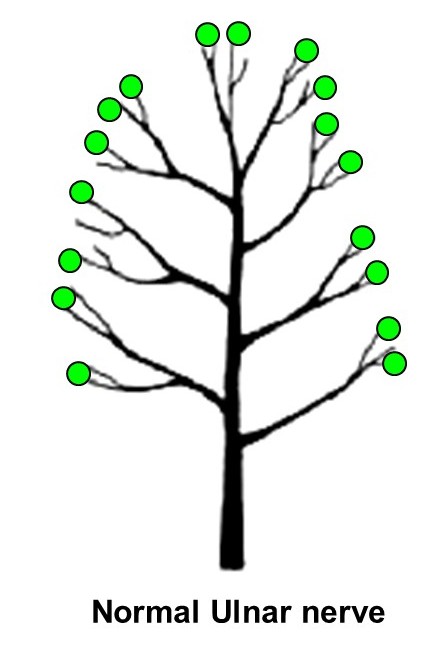
The nerves supplying sensation and controlling muscles in the hand start in the neck and travel down the arm. The ulnar nerve can be compressed at many levels but commonly at the elbow.
- Neck ( Cervical Spine)
- Thoracic Outlet ( Brachial Plexus)
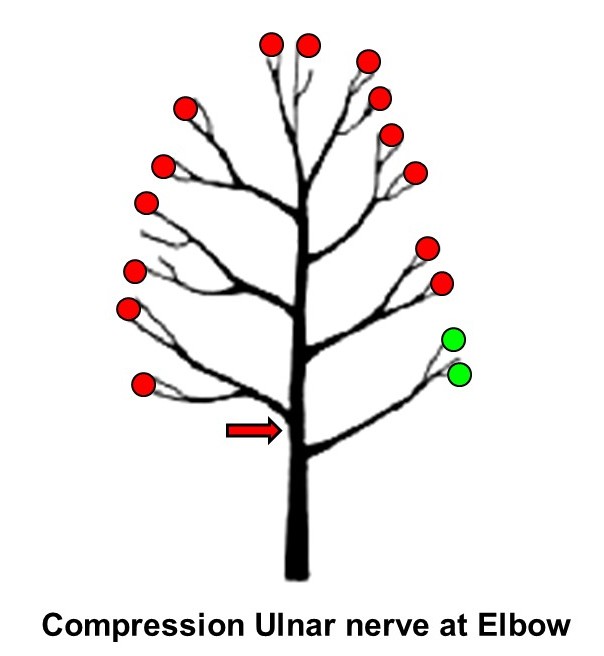
- Elbow ( Cubital Tunnel)
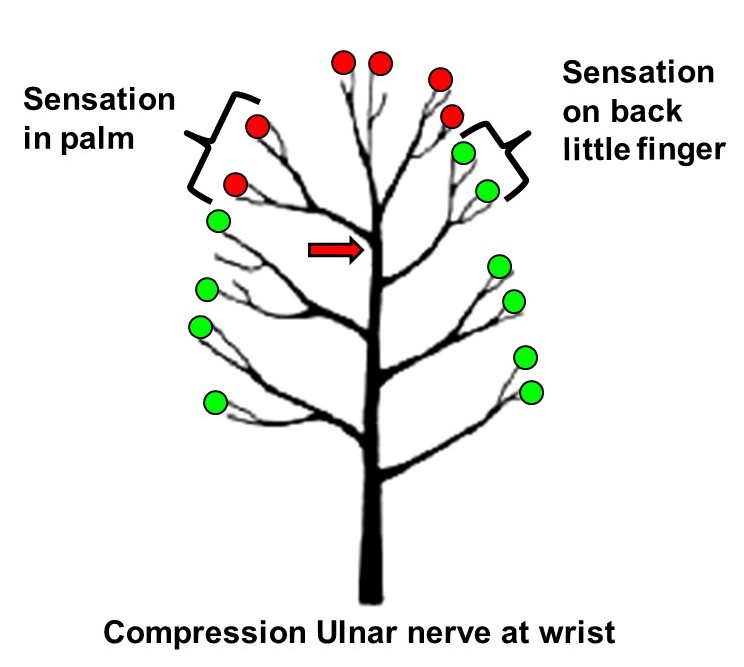
- Wrist ( Guyon's Canal)
Many people have hit their so called “Funny bone” causing significant temporary pain on the inside of the elbow and tingling in the hand. The “funny bone” is not really a bone – it is the Ulnar nerve.

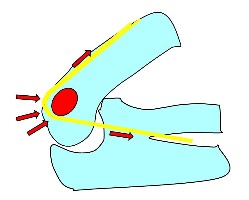
The Ulnar nerve passes behind the elbow through a tunnel ( The Cubital Tunnel).
- Cubital Tunnel Syndrome is usually not a serious problem. If the symptoms are present for a long time or the numbness becomes constant (i.e. present night & day) then it may indicate permanent nerve damage. This may cause permanent weakness and numbness in the hand.
WHAT CAUSES Cubital Tunnel?
- The causes of nerve entrapment are often multifactorial.
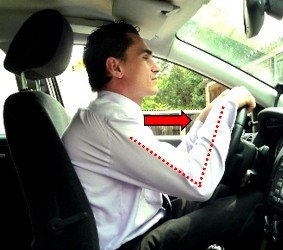
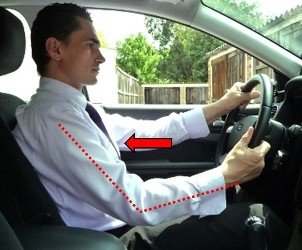
Cubital tunnel syndrome may happen when a person bends their elbow, leans on their elbow frequently or has an injury to the area.
Other factors include:
- Age
- Genetics
- Elbow posture - eg playing Cello
- Leaning on elbow
- Trauma - Lacerations , fractures, heterotopic ossification
- Arthritis - Flexed posture, Spurs
- Ganglions
- Anatomical variations
- General
- Smoking – (? reduces blood flow to nerve)
- Alcohol - Lifetime intake
- Drugs eg Arimidex
- Diabetes
- External pressure - Casts , Prolonged surgery , Prolonged Bedrest
- Elbow deformity - Valgus or Varus


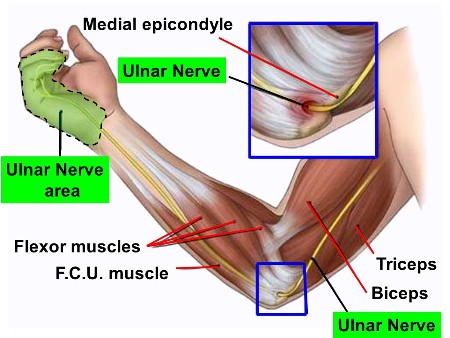
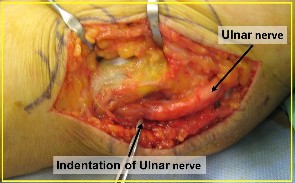
Ulnar nerve Anatomy
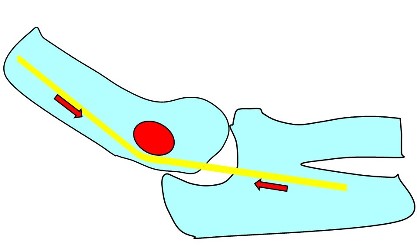
The Ulnar nerve passes from the front to the back compartment of the arm piercing a fibrous band (Arcade of Struthers) ~ 10 cm above the elbow ( medial epicondyle) . It then enters the Cubital tunnel. The nerve can be felt with your fingers behind the bony prominence on the inside of the elbow. In some people it flicks over the bone when the elbow is bent.
The Cubital tunnel is made up of:
- a roof – the FCU fascia and Osborne's ligament (travels from the medial epicondyle to the olecranon = point of the elbow)
- the floor - formed by the ligament and elbow capsule and
- the walls - formed by medial epicondyle and olecranon. See diagram.
The Commonest Sites of entrapment
- Between the two heads of FCU
- Arcade of Struthers (hiatus in medial intermuscular septum)
- Between Osborne's ligament and MCL
Symptoms
- Numbness & tingling in the ring & little finger especially with elbow flexion
- Numbness and tingling at night
- Sometimes aching pain on the inside of the elbow or fingers
Later
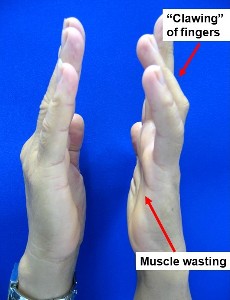
- weakness , incordination with fine manipulation eg buttons
- Clawing of fingers
Precipitating activities
- Telephone use (excessive flexion)
- Sleeping with arm in flexion
- Leaning on forearm on edge chair or desk
Diagnosis:
- The diagnosis is usually straight forward and is made after eliciting a typical history and an examination.
- One can determine the level of nerve compression by identifying which muscles are involved or which areas of the hand have reduced sensation
- Sometimes an ultrasound or nerve conduction tests are performed if the diagnosis is unclear.
- At times it may be difficult to determine if the nerve issue is occurring at the neck , thoracic outlet, elbow or wrist . Occasionally an injection of Cortisone into the cubital tunnel may help differentiate between these causes of nerve compression.
- A positive response to treatment modalities eg a Elbow brace or towel around the elbow may help confirm the diagnosis.
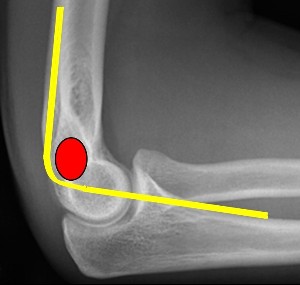
- X-ray elbow if decreased range of motion. This is done look for arthritis or bone spurs.
Treatment:
- Identify treatable causes for the condition
- Activity modification & education
- Most important.
- Stopping any activity that aggravates the condition, such as bending the elbow or reading in bed
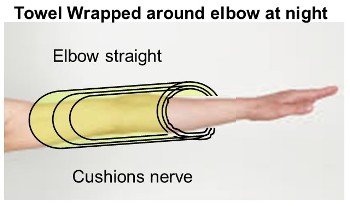
- Night elbow extension splinting
- use towel wrapped around elbow with stocking over the top to hold in place
- Prevents elbow flexion
- Cushions the nerve
- Nerve gliding exercises – See Hand Therapist

- Gel pad on hard surfaces eg desk to cushion ulnar nerve

- Steroid injections under US control – diagnostic & treatment
Surgery:
- Cubital tunnel release is only a moderately effective procedure ( 75% operation) in relieving the symptoms. In contrast Carpal tunnel surgery is a 90- 95% operation.
- Recovery periods are extremely variable.
- If the symptoms are intermittent then many people notice resolution of their nerve symptoms immediately after the operation.
- If the numbness is constant then the sensation may never fully recover or may recover over a prolonged period of time 12 - 18 months.
- Muscle wasting may never fully recover.
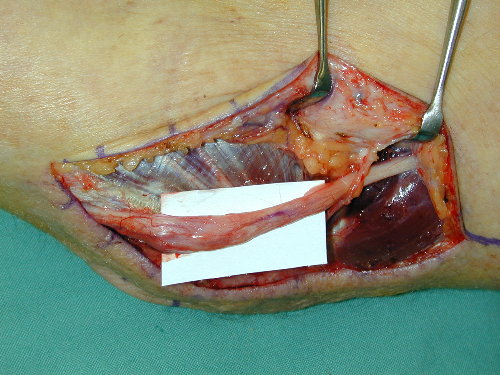
- 1. Decompression
- releasing all the tissue over the nerve. Commonest
- 80-90% good results when symptoms are intermittent
- poor prognosis correlates with muscle wasting
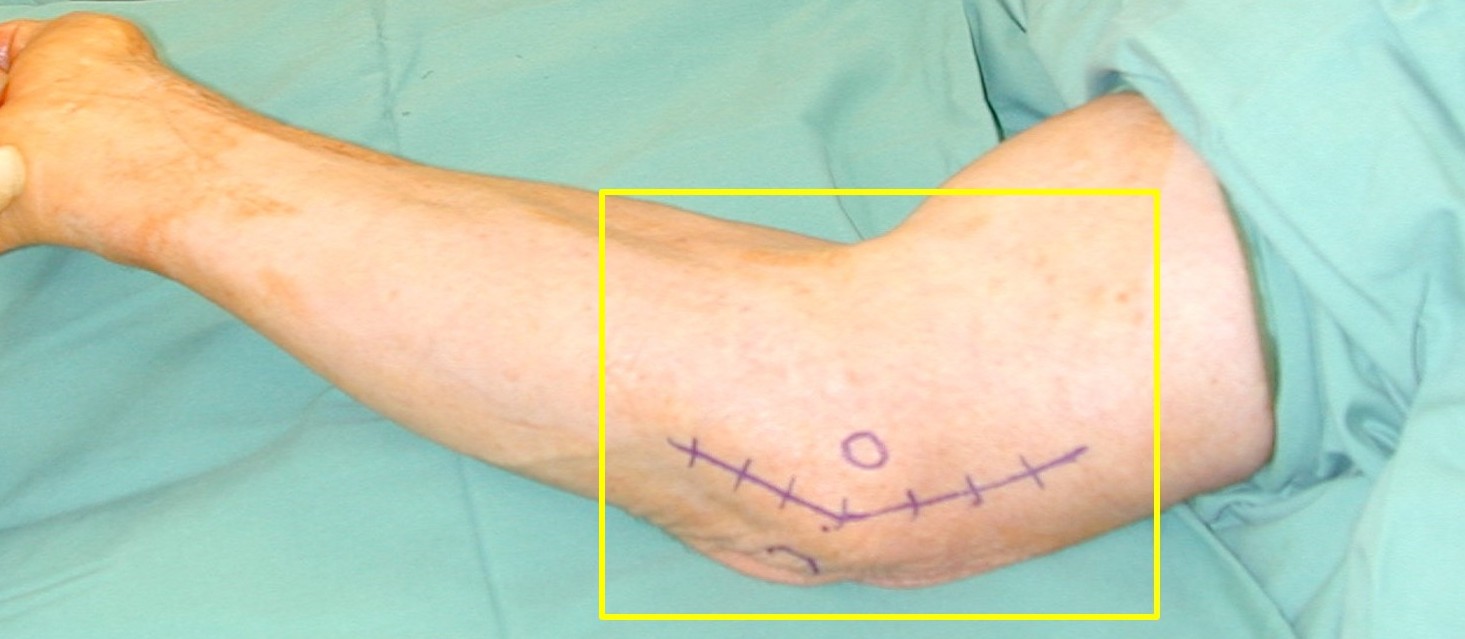
- 10cm incision

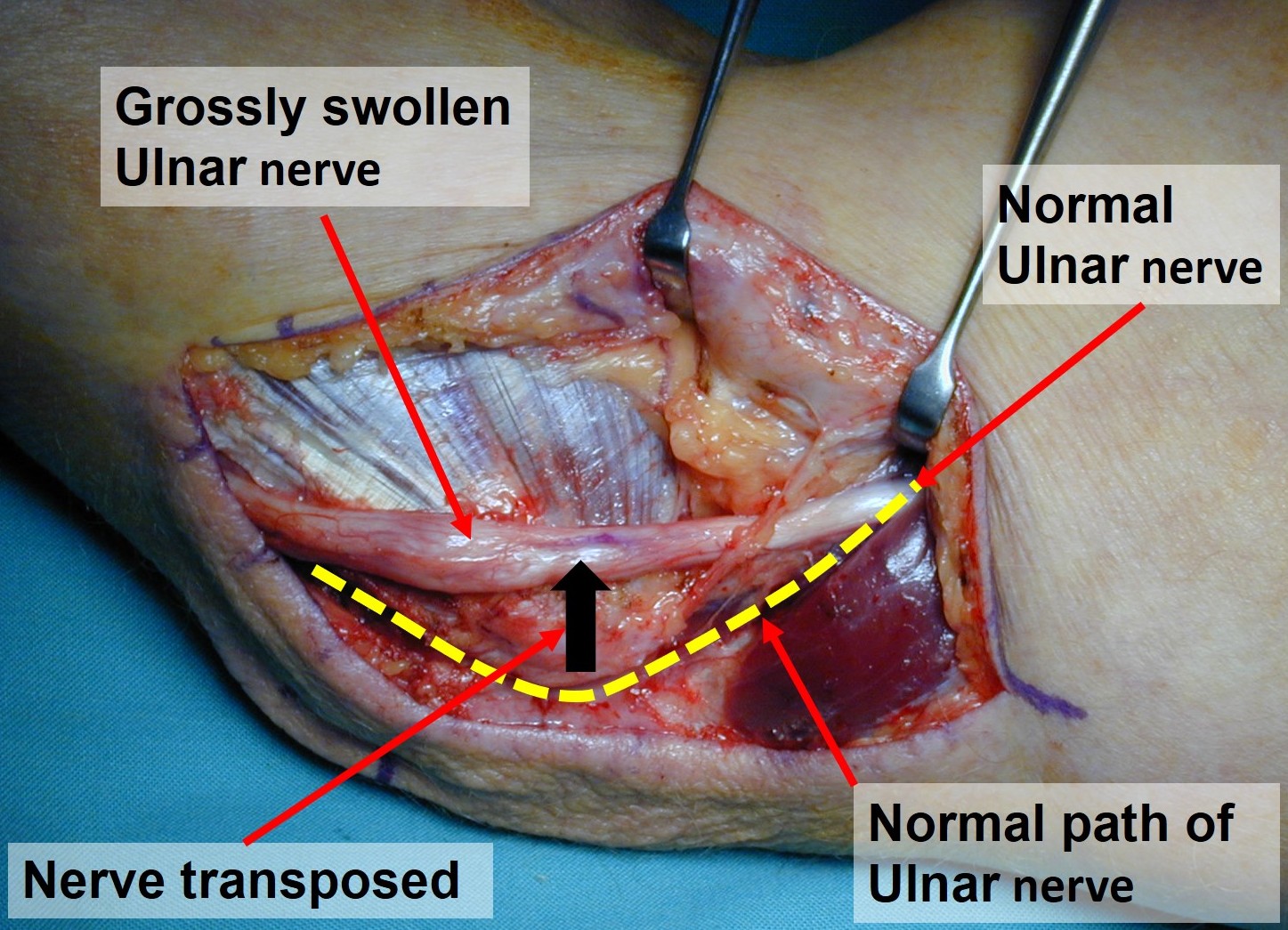
- 2. Decompression + nerve transposition
- Subcutaneous, Sub muscular
Complications of Surgery: See General Hand Surgery Complications
- Failure to regain ulnar nerve function
- Recurrence due to nerve scarring, or tethering to local tissue
- Forearm skin Neuroma formation – scar hypersensitivity or numbness adjacent to scar
- Elbow pain