Thumb Anatomy:
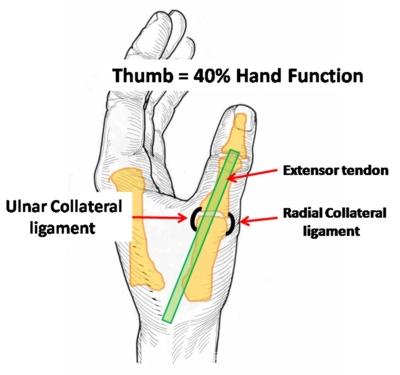
The thumb represents 40% of the hand function. A problem with the thumb can therefore cause significant hand dysfunction.
The priorities in the thumb are that:
1. The thumb is Stable
2. The thumb is Painfree.
An understanding of the complex thumb anatomy will help understand Skiers thumb injuries. I have divided the anatomy into sections including:
1. Joints
2. Bones
3. Ligaments
4. Tendons & Muscles
5. Nerves
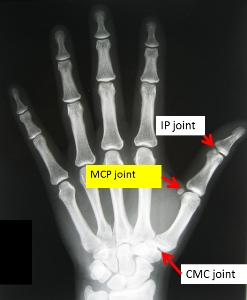
1. Joints:
The middle joint of the thumb is known as the M.C.P. joint ( Metacarpo-phalangeal joint) and is the joint affected in Skier’s thumb injuries.

2. Bones:
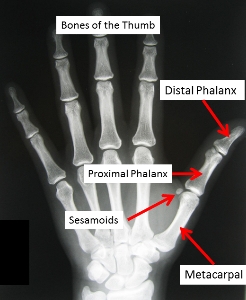
There are 3 main bones in the thumb.
- Metacarpal
- Proximal phalanx
- Distal Phalanx
Skiers thumb injuries occur at the MCP joint between the Metacarpal & Proximal phalanx.
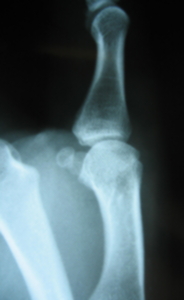
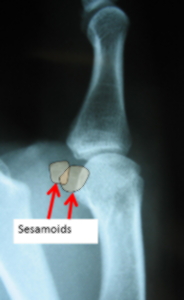
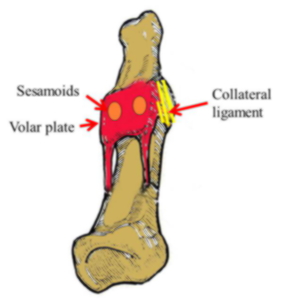
There are often additional small bones on the palm side of the MCP joint known as the Sesamoids.
They are often mistaken for fractures.

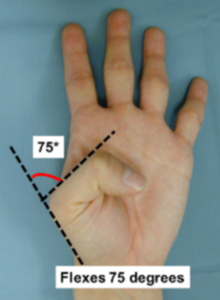
Movement in the thumb is not nearly as critical as it is in the fingers. The range of movement at the MCP joint of the thumb varies greatly between individuals. Some have an arc of movement of only 30*, others an arc of nearly 180*. The differences are due to the shape of the joint surface.
"Round head" "Square head"
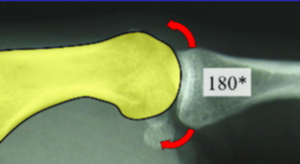
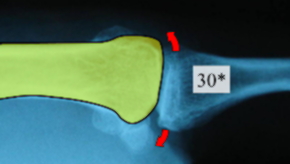
More movement does not equate with increase in function and hyper-extending at this joint may be disadvantageous.
3. Ligaments:
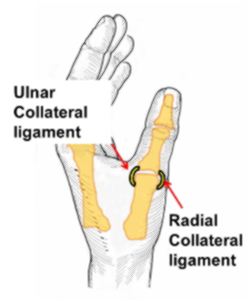

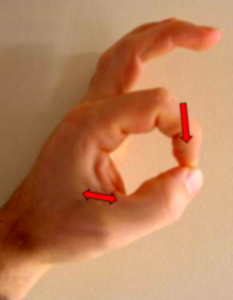
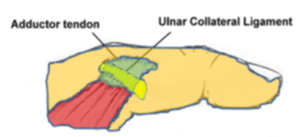
The M.C.P. joint is surrounded by a capsule. Thickenings of the capsule are called ligaments. The M.C.P. joint has 2 main collateral ligaments on the sides of the joint. These stabilize the joint preventing excessive side - to - side motion. The Ulnar collateral ligament is the most important of these because every time one grasps objects between the thumb and index finger this ligament stabilizes the thumb. Loss of this ligament results in significant pinch strength weakness.
The collateral ligaments are divided into 2 components.
1. The Proper Collateral ligament – extends from bone to bone
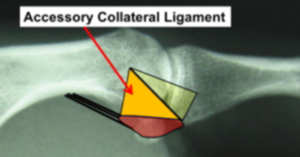
2. The Accessory Collateral ligament – extends from bone to the volar plate.
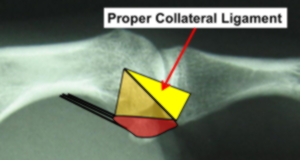
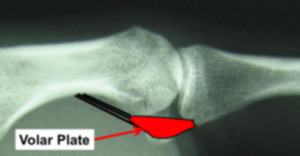
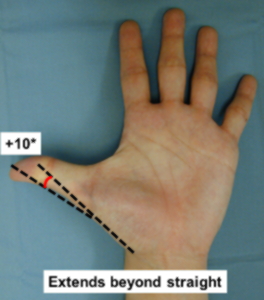
The Volar plate is a very strong fibro-cartilaginous structure on the palm side of the joint which limits thumb extension.
The volar side of a bone or joint refers to the palm side of the joint. ( Volar = Palm side)
Embedded within the volar plate are 2 round bones ( Sesamoids) which are often mistaken as fractures on thumb X-rays. Extending from the volar plate proximally are 2 Check ligaments.
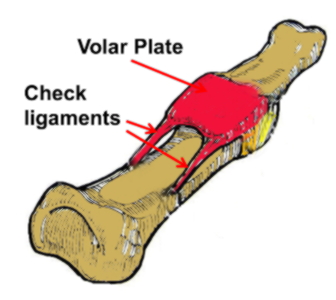
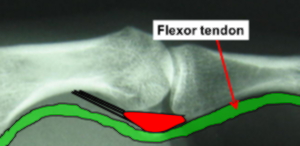
The volar plate also acts as a spacer between the joint and the flexor tendon.
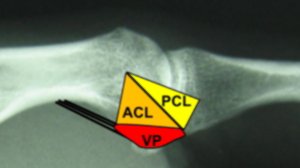
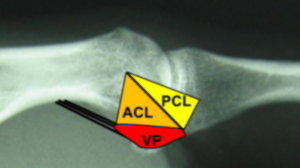
In essence the collateral ligaments and the volar plate are like 3 sides of a box.
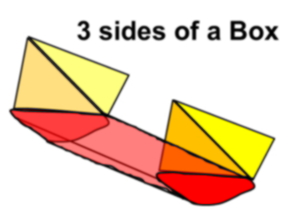
This makes sense as one does not want the thumb to wobble from side - to - side or bend back excessively but it is desirable for it to bend. The capsule on the back of the joint is therefore much thinner.
4. Tendons / Muscles:
On the back of the thumb are 2 extensor tendons ( EPL & EPL tendons) which act to straighten or extend the thumb . They form a broad tendon expansion. These tendons are gently retracted at the time of surgery to gain better access to the thumb MCP joint. As there is a broad tendon surface there is significant potential for the tendons to stick down to the underlying bone after surgery resulting in limitation of movement at the Interphalangeal joint.
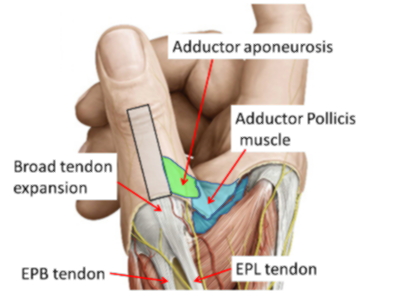
Attaching to the side of the EPL tendon is the Adductor aponeurosis. This is a broad but thin tendon expansion which joins the adductor pollicis muscle to the EPL tendon. The adductor muscle arises on the palm side of the hand from the middle metacarpal bone. It is a critical structure in understanding the pathology of Stener lesions in Skier’s thumbs. The adductor tendon lies over the top of ( superficial to) the Ulnar collateral ligament.

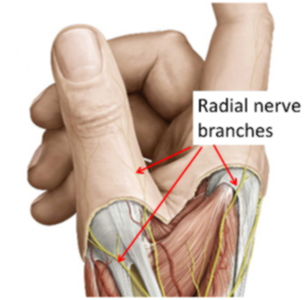
5. Nerves:
There are multiple branches of the Superficial Radial nerve running along the back & sides of the thumb. During surgery these are identified and retracted. The very act of retraction on these nerve branches can make the scar tender for a while after surgery.
LAST UPDATED ON 13 / 4 / 2015