Childrens Hand Fractures
Dr Stuart J.D. Myers
MB BS Hons (NSW), FRACS, FA(Orth)A
www.myhand.com.au
General
Many people think that a “fracture” is different from a "break”, but they are the same.
Effect on the hand
The forces causing a fracture may also injure other structures such as muscles, tendons & ligaments and in children the finger nail.
When a bone breaks there is bleeding from the bone ends. Bleeding leads to scarring which results in stiffness particularly in the fingers. While this is a common problem in adults it is not common in children.
Childrens fractures can be immobilised in a splint for 3 – 6 weeks and they often regain range of motion very rapidly when the splint is removed.
If a fracture involves the joint surface then arthritis may develop later in life.
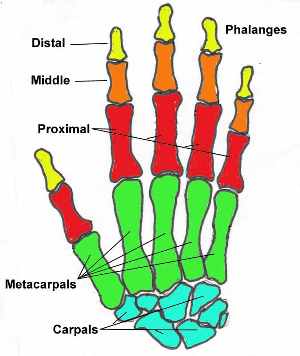
In children’s bones the “weak link” is the growth plate. This is formed from cartilage and appears as a dark line on the xray. The cartilage multiplies and is then converted into bone. In this way the bone increases in length.


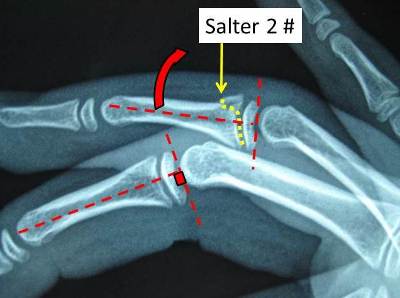
Growth plate injuries are subdivided according to the Salter – Harris Classification. The higher the number the greater the risk of damage to the growth plate and the greater risk of problems. In reality a “growth arrest” is VERY uncommon.
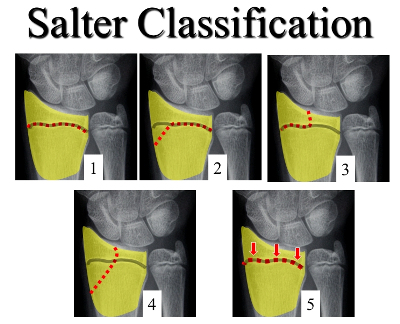
Consequences of Growth plate injury:
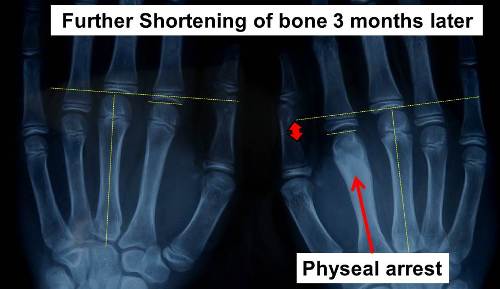
1. Shortening – If the entire growth plate is damaged. ( ~50% Salter 5 fractures) rare in others
2. Progressive bending of a bone if part of the growth plate “arrests” but the remaining growth plate continues to grow.
3. Joint surface irregularity - if a Salter 3 or 4 fracture
Fracture Issues
There are many issues to take into consideration in the management of these fractures.
Age
Time remaining before growth ceases
Dominant Hand Non Dominant Hand
Stable Unstable
Undisplaced Displaced
Acceptable Unacceptable deformity
Displacement - Rotation
- Shortening
- Bent
Joint involvement - Step ___ -----
- Gap ___ ___
Bone quality - Osteoporosis
Number bone fragments - comminution
Growth Plate involved Not involved
Other injuries eg nerve, tendons, ligaments
Acceptable Unacceptable
Risks of Surgery v Risks of No surgery
Fixable Not Fixable

Need for Xray monitoring No Follow up
Treatment Principles:
1. Reduce Swelling - ice packs,
- elevation
- Coban bandage
2. Control Pain - splint, pain killers
3. Prevent Stiffness - early movement if the fracture is stable (even before the fracture has healed)
4. Stabilise the unstable
5. Correct Deformity - Rotation
- Angulation
- Shortening
- Joint step - prevent arthritis
Options:
- Coban bandage / Buddy strapping / Early movement




- Closed Reduction & Splint - pulling on the bones under an anaesthetic to realign the fracture


- K Wires


- Plates & Screws ( Rare)
- Xray monitoring - a growth arrest may only reveal itself over time and so monitoring may be required for a year or 2. 
“Reduction” means pulling the bones back into place. This can be done “Closed" in which no cut is made & a plaster or splint is applied or “ Open” where a cut is performed &
the bones are directly repositioned .An open reduction often requires the use of wires, plates & screws.
Results
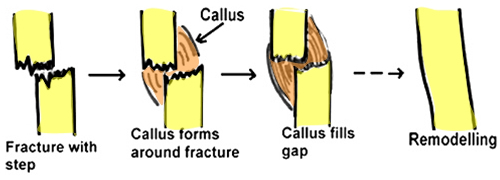
- Perfect alignment of the bone on X-ray is not always necessary to get an excellent result. A bony lump may appear at the fracture site as the bone heals & is known as “fracture callus”. This is a normal part of the healing process & usually gets smaller over time.
- The growth plate has the potential to correct deformity in the plane of movement of the finger. Ie the growth plate may grow on the crushed side of the bone quicker than the opposite side and thus correct malalignment.
It will not correct deformity from side to side or malrotation.


- Occasionally loss of bone alignment occurs & additional treatment may be required
- In general it takes 3 - 6 weeks for a hand fracture to heal depending on the age. The younger the faster a bone heals.
Revised 10 / 9 / 18