

General:
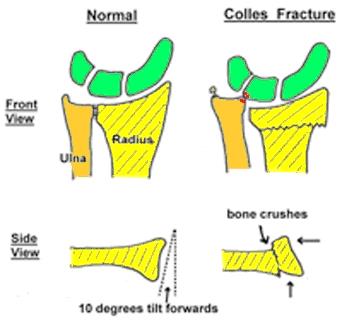
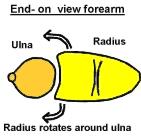
This is the commonest wrist fracture & often occurs in postmenopausal women. It usually results from a fall onto the outstretched hand & leads to the Radius (larger forearm bone) crushing into itself & tilting backwards.
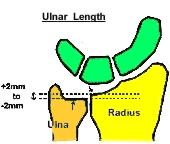
A Colles fracture results in the radius shortening or conversely the ulna becomes too long and impacts against the wrist bones.
Normally the radius is tilted forward approx. 10 degrees on a side view.
On a front view of the wrist the radius and ulnar are approximately the same length. Normal Wrist Anatomy





Issues:
There are many issues to take into consideration in the management of this fracture.
Any given Colles fracture may be well treated in several different ways.
- Age, Activity Level, General Health
- Non - Dominant Hand Dominant Hand
- Undisplaced Displaced
- Joint surface Involved - Step __---- in joint surface
- Gap ---- ---- in joint surface
- Comminution (1 fragment or many fragments)
- Osteoporosis (Soft bones)
- Growth plate involved (children)
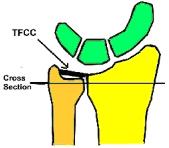
- Other injuries eg nerve, cartilage, ligaments
- Stable Unstable
- Acceptable Unacceptable
- Fixable to allow immediate movement
- Risks of Surgery
Treatment:
The aim is to hold the fractured bones in a satisfactory position until healing occurs (usually in a plaster cast for 6 weeks) and avoid complications along the way.
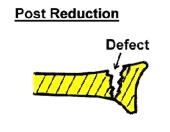
If the fracture is displaced then a “Closed reduction” may be required (pulling on the bones under an anaesthetic to realign the fracture).
If the fracture is very unstable additional measures may be required to stabilise the fracture (“ Open reduction”) Operation Technique
- Plates
- Screws
- Wires
- External Fixateurs
- Bone graft from the hip
- Bone substitute


Sometimes the best long-term functional result is achieved by accepting a degree of deformity and starting early movement once the fracture has healed. One has to balance the advantages versus the risks of an operation and this is a decision that requires considerable experience.
Plaster:
The arm should be comfortable in the cast. If it feels uncomfortable despite Panadol and elevation; or if the cast feels too tight then let your doctor know immediately. While in the cast it is important to exercise the fingers, elbow & shoulder to prevent stiffness.
The arm may be X-Rayed regularly if the fracture is unstable to make sure that the fracture position does not change. The outer bandage around the half plaster slab needs to be tightened regularly so that the plaster feels snug but not too tight.

After plaster removed:
Your doctor will give you a Tubigrip bandage for comfort. This can be removed for showering or when no longer required for support.
Perform finger & wrist exercises & grip strengthening exercises squeezing putty or a squash ball.
It is not uncommon to experience some discomfort for a few months in the wrist especially on the side away from the thumb. This usually settles with time.
Do not do any heavy lifting or play sport for 6 weeks after the plaster is removed.
Do not return to driving until you can turn the steering wheel in an emergency.
Complications:
1. Swelling – plaster too tight
2. Malunion – angled, shortening
3. Complex Regional pain syndrome (CRPS)
4. Nerve entrapment eg Carpal Tunnel
5. Tendon rupture
6. Arthritis
7. Other
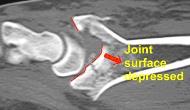
Examples:
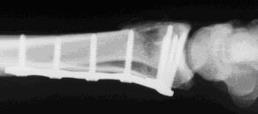
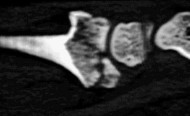
A 27 year old snow boarder falls at high speed. The Xrays tend to understate the injury. There is not only a Colles fracture with an associated fracture at the base of the ulna styloid but also a Scaphoid fracture. The degree of joint surface disruption and degree of comminution ( multiple fragments) is best seen on the CT scan.

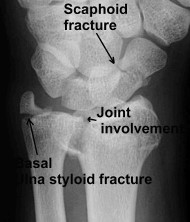
Front view Xray

Side View Xray
CT Scan reveals scaphoid fracture CT Scan side view

Internal fixation of all fractures allows immediate movement of the wrist and no cast


A removable brace is used in the early post-operative period for comfort.

At 8 weeks satisfactory movement after a significant wrist injury.



At 5 months the movement was ~ full.


Example 2:
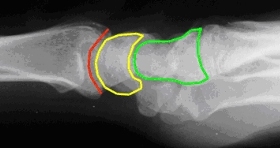
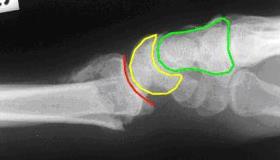
Normal alignment Colles fracture with change in wrist alignment
A Colles fracture alters the alignment of the small bones (within the wrist). This can result in arthritis throughout the wrist.
Example 3:


A fracture involving the joint surface with a large step will result in rapid onset arthritis if left untreated.
Revised 6 / 10 / 06
LAST UPDATED ON MONDAY, 08 SEPTEMBER 2008 15:49