

General:
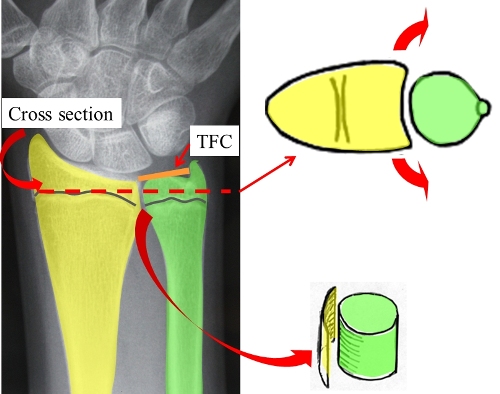
There are 2 bones in the forearm. The Radius and Ulna bones are approximately the same length. ( See diagram below)
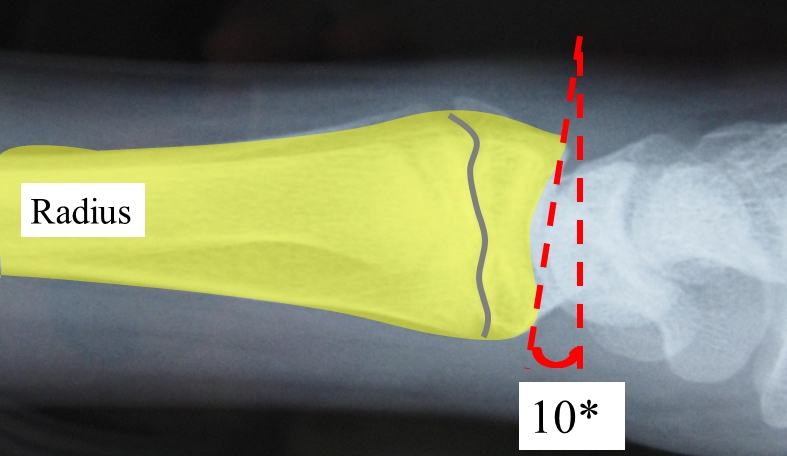
Normally the radius is tilted forward approx. 10 degrees on a side view x-ray of the wrist.
A fracture of the distal radius is the commonest fracture. It usually results from a fall onto the outstretched hand & leads to the Radius (larger forearm bone) crushing, tilting or displacing backwards.
Normal Wrist X-rays
Front view Side View
Hand Xray

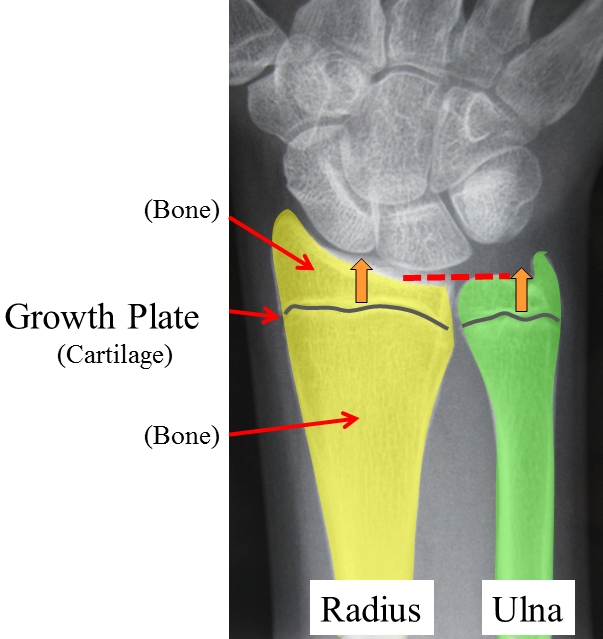
NB multiple growth plates
Children’s bones differ from adults.
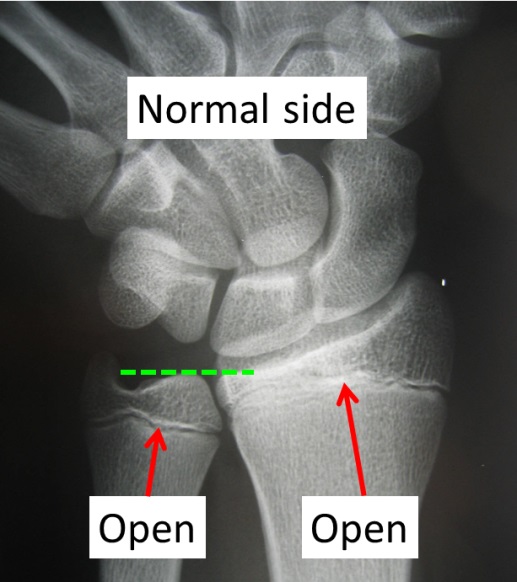
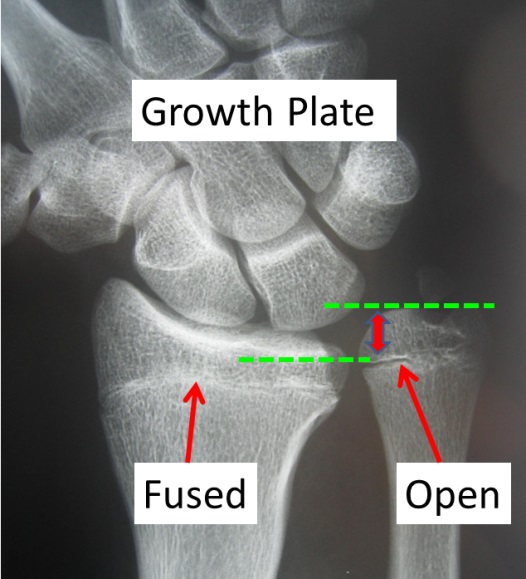
1. They have growth plates which allow the bones to increase in length. These are seen as dark lines on the x-rays. All the finger bones have growth plates as do the forearm bones. The growth plate is made up of cartilage and so does not show up on an X-ray. It is confusing because the joint surfaces are also covered with a different type of cartilage. ( This also does not show up on x-rays and so the joints also appear as gaps on the x-rays.)
The growth plates in the forearm often close at age 16 in girls and 18 in boys although this is highly variable when you reach “skeletal maturity.” ( ie stop growing!) The growth plate (or physeal plate) is the weak link in the chain and so many fractures occur at this level.
2. Children’s bones are more flexible and may bend rather than break. Adult bones are stronger but relatively brittle so they break rather than bend. Dislocations are rare in children because their ligaments are stronger than bones in general.
3. Childrens bones have the potential to remodel with growth.
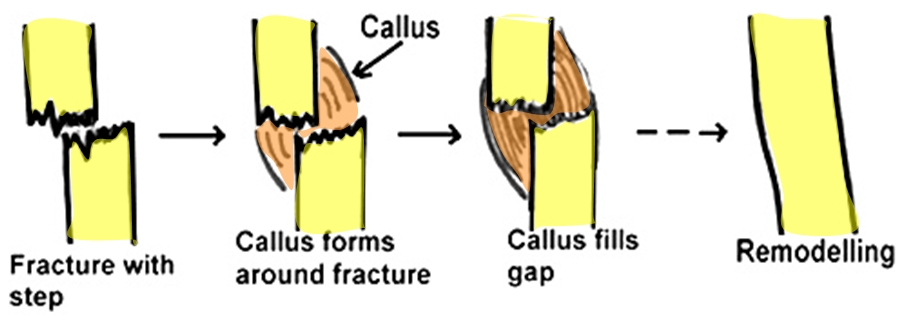
1.Torus fracture – Often difficult to see on Xray. Is a partial fracture or buckling of one side of the bone. This fracture often heals in 1 – 2 weeks depending on the age of the child. The treatment is to make the wrist comfortable either in a splint or a cast.


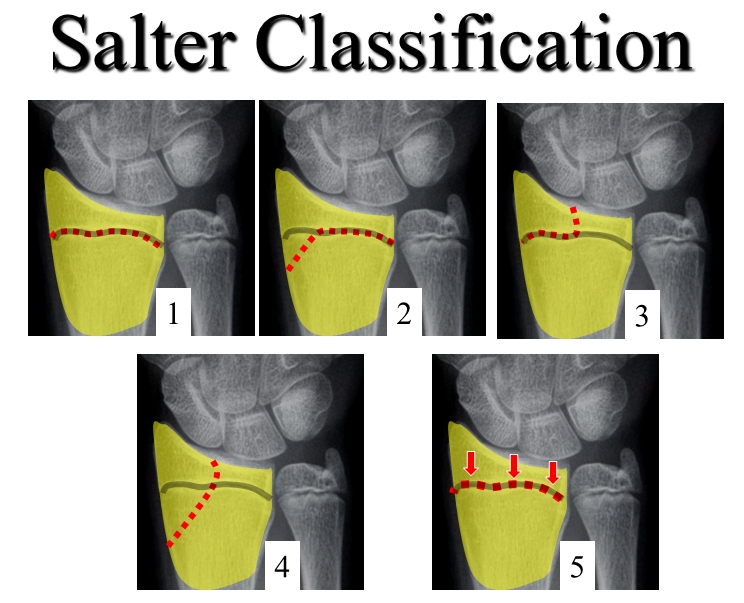
2. Growth plate fractures are also very common injuries. They are significant in that they can result in permanent damage to the growth plate which in turn can result in progressive deformity as the child grows. Thankfully “growth arrest” is not common but it needs to be monitored for with xrays taken for a prolonged period of time after the fracture heels depending on the fracture type. The Salter-Harris classification system is detailed below and is based on the pattern of fracture as it extends either across or through the growth plate.
Consequences of Growth plate injury:
For an individual bone a growth plate injury can cause:
1. Shortening – If the entire growth plate is damaged. ( ~50% Salter 5 fractures) rare in others
2. Progressive bending of a bone if part of the growth plate “arrests” but the remaining growth plate continues to grow.
3. Joint surface irregularity - if a Salter 3 or 4 fracture
4. In the forearm ( a 2 bone system) if the radius growth plate arrests then the ulna can become progressively too long.
Example: Salter 2 displaced radial fracture.


The fracture was treated with a “Closed Reduction” under anaesthetic. The fracture is manipulated back into place.
Issues:
There are many issues to take into consideration in the management of these fractures. Any given Distal Radial fracture may be well treated in several different ways.
Age
Time remaining before growth ceases
Non - Dominant Hand
Undisplaced Displaced
Growth plate involved
Joint surface Involved - Step __----
- Gap ---- ----
Comminution (Many fragments)
Stable Unstable
Other injuries eg nerve, cartilage, ligaments
Acceptable Unacceptable
Risks of Surgery v Risks No surgery
Need Re – Xray
Treatment Options:
- Plaster
- Closed Reduction & Plaster
- Wires
- Plates & Screws
The aim is to hold the fractured bones in a satisfactory position until healing occurs (usually in a plaster cast for 3 - 6 weeks) and avoid complications along the way.
If the fracture is displaced then a “Closed reduction” may be required (pulling on the bones under an anaesthetic to realign the fracture).
Initially a half plaster is applied to allow for swelling that inevitably occurs for 24 – 72 hours after the fracture.

After 1 – 2 weeks a full waterproof cast can then be applied. If a closed reduction has been performed the position of the fracture must be carefully controlled while the cast is being changed. After cast change repeat X-rays are performed.

If the fracture is very unstable additional measures may be required to stabilise the fracture (“ Open reduction”).
Sometimes the best long-term functional result is achieved by accepting a degree of deformity and starting early movement once the fracture has healed. One has to balance the advantages versus the risks of an operation and this is a decision that requires considerable experience.
Plaster
The arm should be comfortable in the cast. If it feels uncomfortable despite Panadol and elevation; or if the cast feels too tight then let your doctor know immediately. While in the cast it is important to exercise the fingers, elbow & shoulder to prevent stiffness.
The arm may be X-Rayed regularly if the fracture is unstable to make sure that the fracture position does not change. The outer bandage around the half plaster slab needs to be tightened regularly so that the plaster feels snug but not too tight.
After plaster removed
Your doctor will give you a Tubigrip bandage for comfort. This can be removed for showering or when no longer required for support.
Perform finger & wrist exercises & grip strengthening exercises squeezing putty or a squash ball.
It is not uncommon to experience some discomfort for a few months in the wrist especially on the side away from the thumb. This usually settles with time.
Do not do any heavy lifting or play sport for 6 weeks after the plaster is removed. Do not return to driving until you can turn the steering wheel in an emergency.
Complications:
1. Swelling – plaster too tight
2. Malunion – angled, shortening
3. Growth plate damage with resultant deformity – Shortening , angulation

4. Complex Regional pain syndrome (CRPS)
5. Nerve entrapment eg Carpal Tunnel
6. Arthritis
A Tubigrip brace is used in the early post-operative period for comfort.
LAST UPDATED ON 30 /3/ 2015