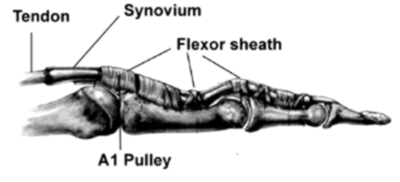
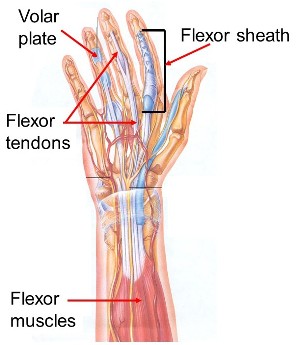
The flexor sheath is a smooth tunnel running up the front of each finger. It holds the flexor tendons down to the underlying bones.
It is like the eyelets in a fishing rod.
There are two tendons per finger running in this tunnel. ( FDS & FDP tendons )
The sheath is lined with synovium which is a tissue which produces the lubricating fluid for joints and tendon sheaths.
Thickenings of the sheath are called pulleys.
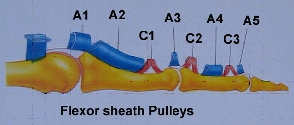
There are two types of pulleys.
The annular pulleys are relatively strong. There are five separate annular pulleys.
The A2 and A4 pulleys are tough and relatively inflexible and arise from the underlying bone.
The A1 , A3 and A5 pulleys arise from the ligamentous tissues ( Volar Plate ) on the front of the respective joints.
The thumb has only two annular pulleys.
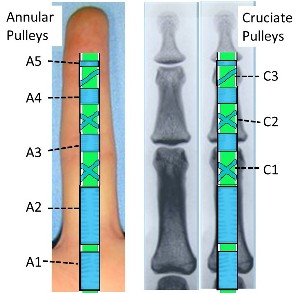
The cruciate pulleys are soft and flexible so that they can get out of the way during finger flexion.
The A2 and A4 pulleys are considered to be the most important.
A Pulley is defined as “A wheel with a grooved rim in which a rope, chain, belt … or tendon can run, in order to change the direction or point of application of a force applied to the … tendon”.
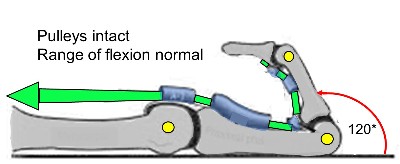
The tendons will always travel in a straight line unless restrained by a pulley. Ie they take the shortest line between the base and the tip of the finger.
See more information re ( Pulley Biomechanics)
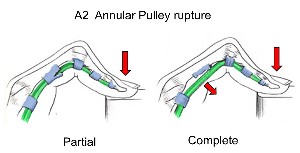
Bowstringing
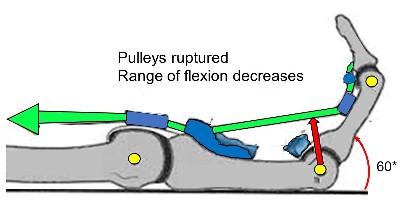
Bowstringing occurs when there is a complete pulley rupture.
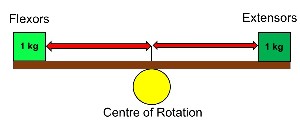
When a finger bends it rotates around the so-called centre of rotation of the joint.
Any tendon which is lying below the centre of rotation is an extensor of the finger and any tendon above the centre of rotation is a flexor. See diagram.
There is a fine balance between the forces of the finger extensor ( straightening ) and flexor (bending ) tendons.
It is similar to the forces on a seesaw.
If the same weight on a seesaw is moved further away from the centre of the seesaw it has a relatively greater effect.
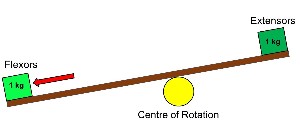
This explains the typical development of a flexion deformity of the finger when there has been a significant pulley rupture.
It also results in loss of full finger flexion. The flexor tendons move away from the joint and although the muscle contraction force has not changed the relative force across the joint has increased.


Most commonly significant bowstringing will only occur if at least two sequential pulleys have been completely ruptured but there have been documented cases of it occurring in isolated A2 ruptures.
Bowstringing leads to flexion contracture of the fingers and grip strength weakness.
Mechanism of Injury
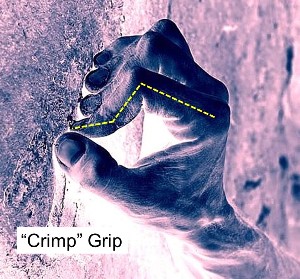
A pulley rupture is commonly seen in rock climbing.
The majority of climbers who have suffered either partial or complete rupture of a flexor tendon pulley describe acute onset while performing a difficult move in the ‘crimp’ position or when they have shock loaded their fingers as they lost their footing.
Diagnosis
- Sometimes a “popping” sensation is felt at the time of injury.
- Bleeding can track down the finger and occasionally result in a secondary trigger finger.
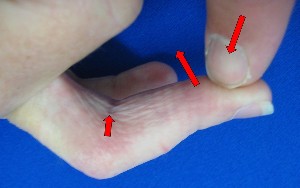
- Swelling & tenderness along palmar side of finger – It is important to document the extent of tenderness.
- Examine for bowstringing. - Resist semi-flexed finger and palpate the front of the finger.
- Place your finger on the tip of the finger and ask them to try and make a fist.
- With your other hand palpate the flexor sheath and feel for bowstringing.
- Always compare with the other side.
- Check for triggering at the A1 pulley level
Investigations
1. Xrays exclude a fracture but rarely confirm the diagnosis.
Very occasionally they may reveal a flake of bone pulled off by the pulley as it tears.
The Xray changes may be subtle and only become apparent after a couple of weeks.

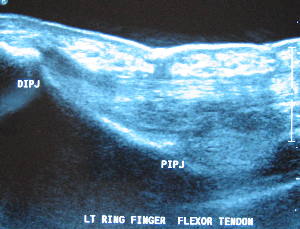
2. Ultrasound
– is absolutely operator dependant
- Allows for dynamic testing with flexion stress on the affected finger.
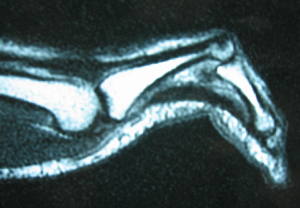
3. MRI scan
Treatment
1. Stop Climbing - for ~ 3 months
2. Splint – by someone with experience in climbing injuries
3. Taping - H Taping ( More Information)
4. Surgery – Pulley repair or reconstruction
Palmaris longus tendon grafts wrapped around the tendon and phalanx are commonly used. There are several techniques involving wrapping the tendon around the phalanx between one and three times.
04 / 08 / 2021