Symptoms:


The injury often occurs skiing when the thumb is bent side ways either by catching in the snow or from the ski stock. It may also occurs in rugby and other sporting injuries. It occurs from a fall on the outstretched hand with the thumb extended. Occasionally it will occur from a steering wheel injury.
Following a typical injury the thumb MCP joint may swell rapidly and is painful. Bruising may develop over a couple of days.
Many patients note weakness when trying to grasp objects. With complete tears the thumb may feel unstable. The severity of the symptoms is not always related to the extent of the initial tear of the UCL. Sometimes partial tears are more painful than complete tears. Simple activities such as tying shoes laces may be difficult. If the thumb catches it may be extremely painful eg putting hands in pocket of pants.
Examination:
The normal thumb is examined first to assess “normal “ ligament laxity and range of motion.
Always check that the “Normal” thumb has not been previously injured!!( These are usually very active people and are often “Repeat offenders”.)
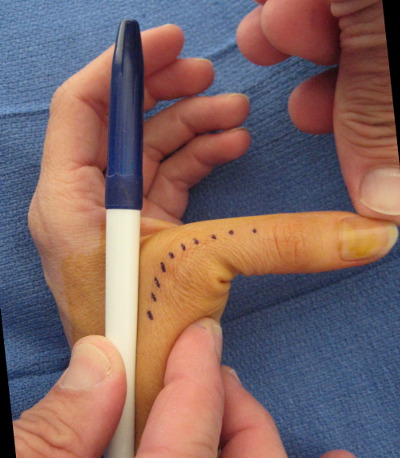
The maximum site of tenderness is noted.
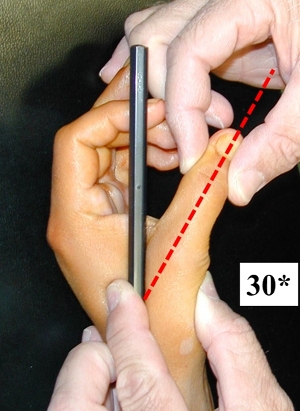
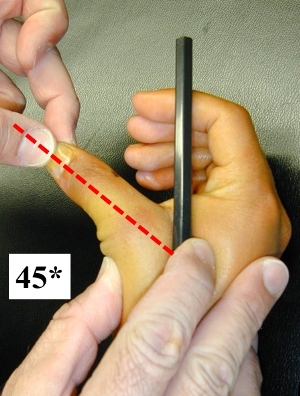
Instability of the MCP joint of the thumb is determined using a pen placed along the thumb and then the thumb is gently stressed in extension and at 25 - 30* of flexion. Test the Radial Collateral ligament first and then the Ulnar collateral ligament last.
After a few days the initial swelling decreases and many Stener lesions can be palpated at this time although this is not reliable.
10 degrees of laxity compared to the opposite side is considered significant. Occasionally the sensation may be reduced along the inner aspect of the thumb due to traction on the nerves at the time of injury.
Grossly unstable thumbs are often not particularly painful to stress.
Investigations:
1. Xrays – are always indicated but may be normal.
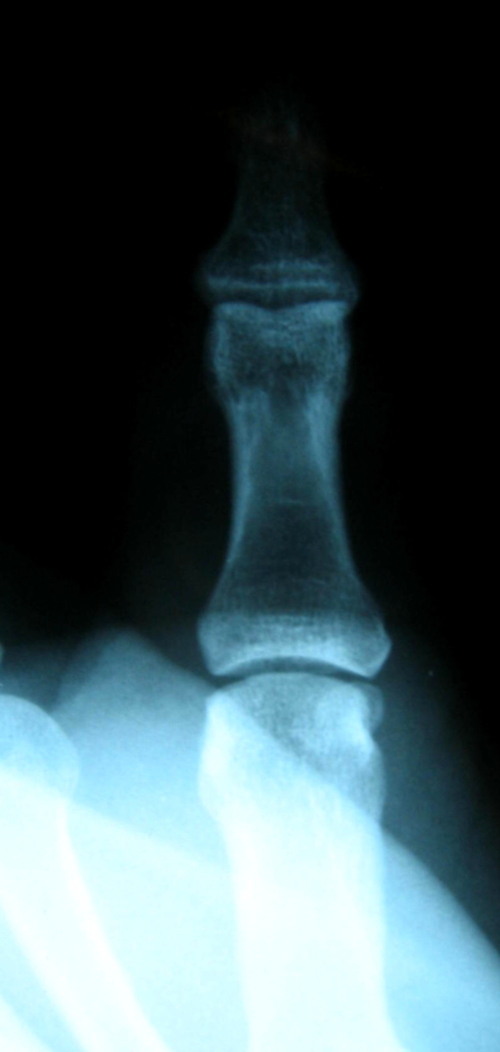



Normal Undisplaced # Rotated # Stener lesion
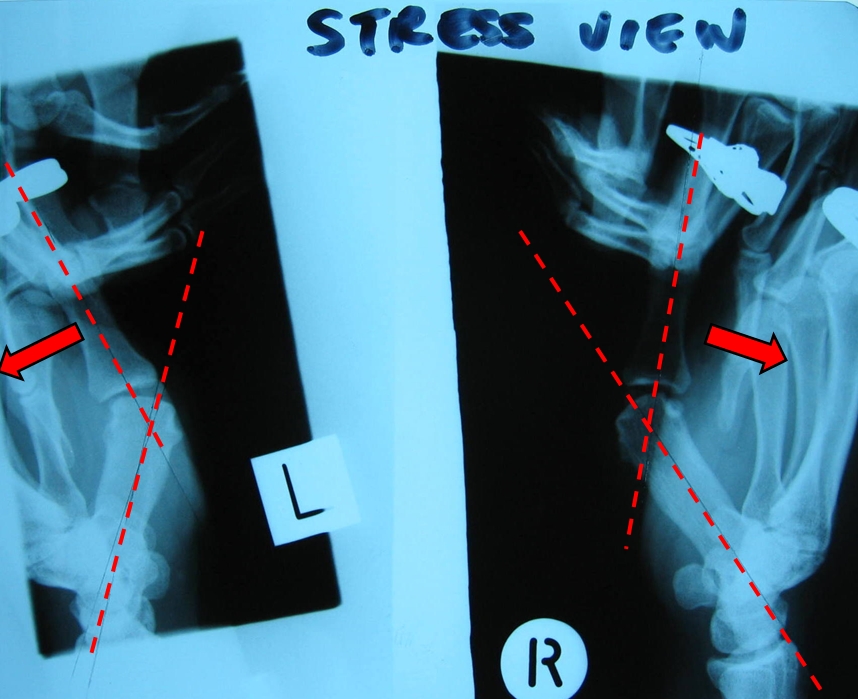
2. Xray Stress Views - Xrays are taken with a deviating stress applied to the thumb.
It is highly operator dependant and while producing “nice” pictures it does not alter my treatment and I rarely perform them .
It is critical to that a “True” AP view of the MCP joint is performed. Slight rotation of the bone can create significant “apparent “ malalignment.
In this case the Radial collateral ligament is being assessed.
3. Ultrasound – Is highly operator dependant and requires a radiologist experienced in Hand Ultrasound. It may demonstrate a Stener lesion but it is poor at differentiating partial from complete ligament tears. I rarely order this investigation. The problem is that often inappropriate investigations delay the onset of appropriate treatment.
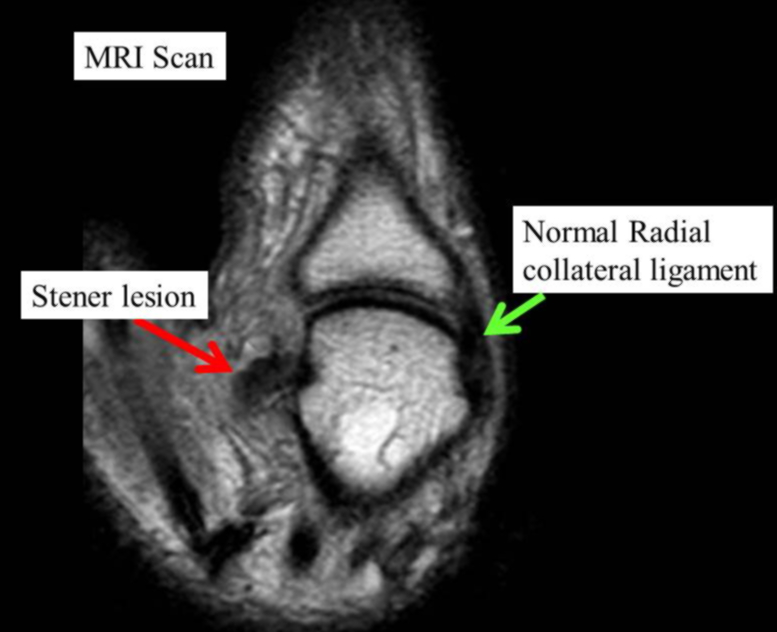
4. MRI Scans- If available urgently may be of assistance in the management of partial ligament injuries but it does not change my management and I rarely perform this investigation. The scan below demonstrates a Stener lesion but this was clinically obvious.
LAST UPDATED ON 14 / 4 / 2015